


In Clay County, Mo., two teenage girls sat together and split a pill.
“One girl took half the pill, and the other one took the other half,” Sheriff Will Akin said. “And the half that had the fentanyl in it — the young girl died, like, right there on the spot.”
It wasn’t supposed to be fentanyl. It wasn’t evenly mixed. But that’s the reality now. Fentanyl isn’t just another opioid — it’s a contaminant, an imitator, a poison. It’s showing up in fake prescriptions, in party drugs, in cocaine and meth without warning.
“You never know what you’re going to get,” Akin said.
That’s what makes it different. There was never a time when using drugs came without any risk. But now, it comes with odds. And in Missouri — where nearly 1,500 people died from synthetic opioid overdoses in 2023 — fentanyl has completely rewritten the math.
The new face of overdose
Dr. Megan Musselman sees the odds play out every day. As Head Pharmacist in the Emergency Department at North Kansas City Hospital, she deals with fentanyl overdoses firsthand — rushing to respond before it’s too late.
“Fentanyl is incredibly potent,” she said. “About 50-100 times stronger than morphine and 25-50 times stronger than heroin.”
That kind of strength isn’t just dangerous — it’s unmanageable.
Often, fentanyl isn’t the only substance involved.
“Many overdose cases also involve other drugs… which complicates treatment,” Musselman said. “For example, fentanyl combined with benzodiazepines or other sedatives can make reversal more difficult.”
But even without the combinations, a dose the size of a grain of sand can shut a body down. And when it’s hiding in something you didn’t plan to take, that tiny dose can be all it takes.
“The presence of fentanyl in non-opioid drugs… increases the risk of accidental overdose,” she said. “Users may not be aware… and they may not have the tolerance for such a potent drug.”
And that’s where things go from dangerous to lethal — fast.
“Overdoses from fentanyl can occur quickly,” Musselman said. “The drug can cause respiratory depression within minutes, and if the person doesn’t receive medical intervention immediately, the outcome can be fatal.”
Sometimes, even minutes are too long.
How local hospitals are adapting to a new drug war
Michelle Lane remembers when fentanyl overdoses were rare.
“In the last five years, the number of patients presenting with an overdose — it was like one or two,” she said. “We had seven on Saturday night.”
Lane is the Senior Director of Community Health and Wellness at North Kansas City Hospital. When fentanyl cases began to spike, she knew the hospital couldn’t just keep reacting — so she shifted her focus to prevention.
“About three years ago, we saw a huge increase… and we were like, ‘We cannot just be, you know, waiting for the people to come to us. We need to do something perfect for prevention.’”
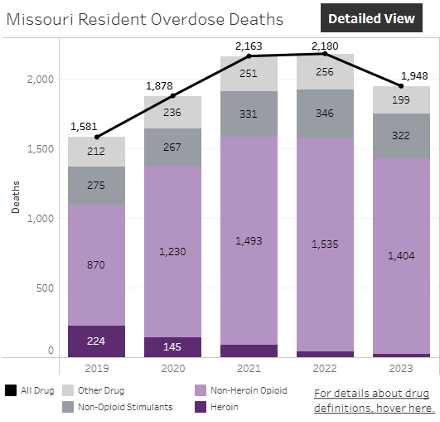
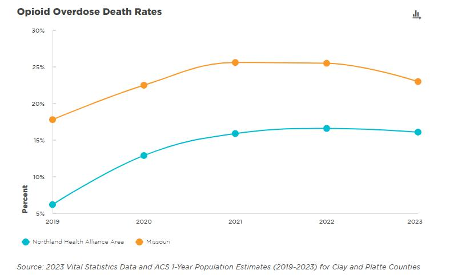
Source: https://health.mo.gov/data/opioids/
So Lane got a grant. And then she got Narcan — thousands of kits. She started in the schools. “I got it into all the high schools,” she said. Then she expanded. “Fire and EMS… the casinos, Clay County Parks and Rec, QuikTrip. We set up a program with Clay County Detention Center… and then they get a Narcan kit too.”
One group, she said, is especially at risk: people just released from jail.
“They don’t use, they come out, they use the same amount that they were using before — and they die.”
Lane has also worked with recovery shelters, tailoring outreach to those who may not realize how vulnerable they are.
“We have people that come in… and they’re like, ‘I don’t mess around with that fentanyl stuff,’” she said. “And I’m like, ‘Okay… well, you quit breathing. And we gave you Narcan.’”
Toxicology reports are often the only thing that convinces them.
“They’re like, ‘I just smoked weed’ or ‘I just did meth,’” she said. “I cannot believe there’s like fentanyl in it. That’s the part that is scary… they just didn’t realize.”
It’s not who you think
“The fentanyl crisis in Kansas City is severe and escalating,” Lane added. “Overdose deaths have surged… The crisis affects all demographics.”
And yet, public perception is stuck in the past.
“These are not dirty, homeless people under the bridge,” Lane said. “These are people with jobs and families and mortgages and nice houses who use recreationally.”
That shift in demographic has forced hospitals to rethink how they flag overdose risk.
“We created a rule… that searched for certain criteria… and gives the hospital provider a task to teach the patient about opioids, Narcan, and offer them a free Narcan kit.”
But stigma, she said, is still the hardest part.
“When a patient comes into the emergency department and they have lung cancer, we feel really sorry for them,” Lane said. “They may have just put their cigarette out before they walked in, but we feel sorry for them. Or somebody comes in and they need diabetes treatment. And why do they need treatment? Because they’ve been eating lemon meringue pie,” she said. “But with those diagnoses, we don’t judge them. We don’t have this statement in our brain. But somebody with a substance misuse disorder?” Lane paused. “People think there’s a dirty feel to them. And that drives me crazy.”
Narcan is the lifeline
Dr. Doug Ham, Medical Director of the Emergency Department, sees the same trend.
“We don’t always know what it is,” he said. “We say fentanyl, but it could be almost anything… there’s a bunch of different versions.”
Sometimes, it doesn’t show up on the screen. “We’re actually part of a study… to figure out what’s actually in whatever they took,” Ham said.
That effort has revealed unexpected mixtures — including tranquilizers.
“So even though we give them an antidote for the fentanyl… they can still have some drowsiness… because we don’t have an antidote for that.”
Still, Narcan is effective — when given quickly.
“It’s kind of amazing how quickly they’ll respond,” Ham said. “In a matter of just seconds.”
But that miracle comes with a cost.
“It kind of puts them into acute withdrawal,” he said. “They’ll wake up… mad, angry, sometimes vomiting.”
Some never get that chance.
Dr. Ham recalled one case that stuck with him — four friends at a party, thinking they were doing cocaine.
“Luckily, only one of them did not snort it,” he said. “The other three did, and it turned out it was an opioid — probably fentanyl — and all three of them basically stopped breathing.”
The one friend who hadn’t used called for help.
“They would’ve died,” Ham said. “But the fourth one called 911, and all three of them survived because of that.”
It wasn’t a matter of addiction.
“They didn’t think they were doing fentanyl,” Ham said. “They thought they were doing coke.”
Fighting on all fronts
For Detective Clay Thompson in Franklin County, the battle isn’t just in hospitals. It’s in homes.
“There’s a lot of the times when we hit some of these houses and there’s kids inside,” he said. “More times than not, the kids are also testing positive for fentanyl.”
He’s especially worried about younger users taking drugs laced with fentanyl at parties.
“I think that’s a big problem,” he said. “There’s now fentanyl analogs to worry about too, like carfentanil, which is 100 times more potent than fentanyl.”
And like others, he credits Narcan for the recent decline in deaths.
“A lot of the overdoses have decreased a lot because of Narcan being so accessible,” he said.
Beyond the badge
Sheriff Akin of Clay County has been in law enforcement for over 22 years and has watched fentanyl devastate his community from every angle — and while he’s faced violent crime and other drug epidemics, fentanyl feels different.
He remembers a time when overdose investigations were near-constant.
“Every time we turned around, we were doing some kind of fentanyl overdose death investigation,” he said. “We found just over a half a pound of fentanyl at one point. That led to other investigations. We were pretty busy.”
He knows not everyone dying is a repeat user.
“I would have to say the majority of our cases are other drugs that are laced with fentanyl — or believed to be laced with fentanyl,” he said. “It’s not like they were out there looking for it. They just didn’t know.”
But some users are.
“There are people out there who are looking for that level of high,” Akin said. “When some drug users hear that somebody has died from a fentanyl or some type of drug overdose, in their mind, they’re not saying, ‘Oh my gosh, I better stay away from that dealer.’ They’re thinking, ‘Oh my gosh, I gotta make my way to that dealer. Get connected. Because he’s got the good stuff.’”
He’s seen how even multiple doses of Narcan sometimes aren’t enough — or don’t produce the result people expect.
“They used five doses of Narcan before this young woman came out of her high,” he said. “And she was so angry… she just ran. She was like, ‘I don’t need you guys,’ and she just left.”
In some cases, law enforcement can’t intervene.
“It’s not illegal to consume drugs,” he said. “It’s just illegal to possess drugs. So if someone is high but doesn’t have anything on them, there was nothing we could do.”
That’s why his department has taken a new approach.
“In our jail, we have Narcan available — not just to potential inmates who use it, but to their families,” Akin said. “We ask, ‘Do you or someone you know use fentanyl? Could you benefit from having Narcan?’ And if they say yes, then we drop two doses of Narcan in their property.”
They’re also installing a Narcan dispenser at the sheriff’s office.
“Whether it’s for a loved one or for themselves,” he said, “we’re never going to change someone’s addiction or their habits — but if we can at least save someone’s life to give them another chance, then we’re going to do everything that we can to be a part of that.”
Not everyone understood that at first.
“People thought that if you had Narcan, or you were giving Narcan, then you were encouraging the use of illicit drugs,” he said. “That’s simply not the case. We don’t want people to use it — but we don’t want people dying either.”
For Akin, the hardest part of the job isn’t chasing down drugs — it’s facing the grief that follows.
“I think the hardest thing is not so much the drug investigation itself, but it’s managing the grief of the loved ones,” he said. “Because people say, ‘Well, whoever overdoses — that’s a them problem.’ No. Not really. It’s a community problem. It’s a societal problem.”
The ripple effect, he said, is what people don’t see.
“Think about how many people that one person knew… how many lives they were involved in. And that’s just one person.”
Sometimes the grief turns into blame.
“They ask, ‘How come you didn’t get this before it got to my child?’” he said. “But law enforcement is a finite resource. We simply cannot do our job as efficiently without the public’s help.”
That’s why he urges community members to speak up.
“If the public’s not telling us where the problems are at because, ‘Well, I’m not a snitch,’ that whole ideology? No,” he said. “If you want your community safe, you have to let us know what’s going on.”
Even families in law enforcement aren’t immune.
“In our community, we had the son of a long-veteran police officer die from a fentanyl overdose,” he said. “Cops aren’t immune. No one is.”
After one community education forum, a mother approached him in tears.
“She said, ‘That was my daughter you were talking about,’” he said. “She almost died, but she’s much better now. And the reason I come to these events is to share her story. Because we’re wealthy. We have the resources. But it still happened to us.’”
Akin still believes things are improving.
“We are in a much better position today than we were, I’ll just say, three years ago,” he said. “There are a lot of agencies working together… law enforcement, fire, EMS, hospitals, public health, mental health organizations, nonprofit organizations.”
But the work’s not done.
“We’ve gained so much ground,” he said. “The problem is still out there. But I really feel like we’re getting somewhere now.”
A dangerous disconnect
All law enforcement and medical professionals interviewed for this story emphasized the same thing: Narcan saves lives.
In an April 28 press release, the U.S. Department of Homeland Security declared that the Trump administration had delivered “the most secure border in American history.” According to the report, fentanyl trafficking at the southern border dropped 54 percent from March 2024 to March 2025, due to Operation Tidal Wave — a surge in border enforcement, mass deportations, and record-setting drug seizures in Mexico.
But while the administration has celebrated its success at the border, it’s also quietly proposed cuts to the very programs that make survival possible at home.
Three federally funded harm reduction efforts — Improving Access to Overdose Treatment, Overdose Prevention, and the First Responder Comprehensive Addiction and Recovery Act — are all on the chopping block. These programs provide Narcan, overdose education, and critical resources to states and cities across the country.
And they work. Not just in Kansas City, not just in Missouri — but nationally.
Michelle Lane, Senior Director of Community Health and Wellness at North Kansas City Hospital, said her team alone has distributed nearly 10,000 Narcan kits in the past few years. “It works in two to three minutes,” she said. You don’t need a medical background. You just need to care.
Care needs funding. And if the proposed cuts move forward, outreach across the country could collapse. Clinics are already closing. Staff are being laid off. In Philadelphia, Unity Recovery scaled back services to 8,000 people per month. In Pennsylvania, a nonprofit that distributed 30,000 Narcan kits per year has shut down.
A Reuters investigation published in April found that synthetic opioid deaths dropped 33 percent from October 2023 to October 2024 — and credited that decline not to border policy, but to expanded Narcan access and community-based harm reduction.
“People will die as a consequence. There’s no doubt about it,” Dr. Rahul Gupta, former director of the White House Office of National Drug Control Policy, told Reuters. “Lives are dependent upon the availability of life-saving medications like naloxone.”
“To cut the entire networks of care that resulted in the drop in overdoses?” said Unity Recovery’s Robert Ashford to Reuters. “It’s so shortsighted. It lacks any strategy.”
The administration’s own health officials have acknowledged the programs’ success. And yet, it is actively trying to eliminate the very tools that saved those lives.
According to documents obtained and verified by Snopes, the Trump administration’s 2025 budget draft includes the full elimination of the three core naloxone-related programs — despite internal acknowledgment that these programs serve the nation’s most at-risk populations. The Department of Health and Human Services confirmed the document’s authenticity but called it “pre-decisional.” A federal judge has since paused the cuts, but the Trump administration is still appealing.
“This is performance,” said Leo Beletsky, a Northeastern University professor of law and health sciences, to Reuters. “A political strategy masquerading as public health policy.”
Meanwhile, on the ground — in schools, jails, QuikTrips, and ERs — Narcan is still doing what it does best: reversing overdoses, buying time, and saving lives. And yet, the administration is trying to eliminate the very tools that saved those lives.
We don’t have time to argue about blame anymore. People are dying. And the difference between life and death can be one person, one dose, one minute. What remains hardest to overcome isn’t policy — it’s stigma.
This isn’t about politics. It’s not even about drugs.
It’s about poisoning. It’s about silence. It’s about how fast you can get to a person’s side with two doses of Narcan.
And it’s about what happens if you don’t.
No one is immune. Not police families. Not wealthy suburbs. Not your kid. Not your friend.
We can’t get into the minds of those who distribute this — but we can choose to prevent and respond to the best of our abilities.
Change only happens if we talk about it. If we fight for access. If we treat overdose like the public health crisis it is — and keep Narcan in the hands of the people who need it most.

